Major Retail Pharmacy
Designing Secure Household Pharmacy Access
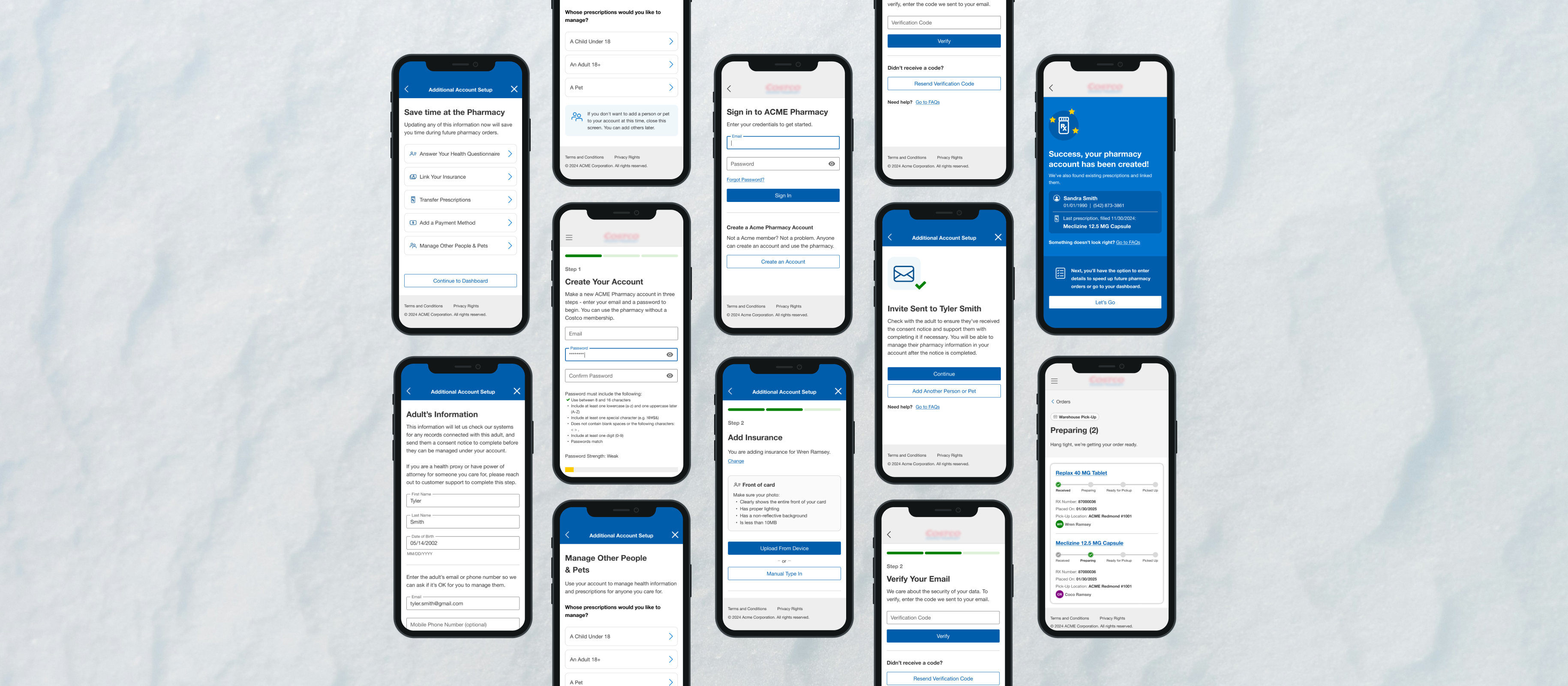
Making identity, consent, and pickup authorization usable under real constraints
Stakes & model
What breaks, who owns what, how the system behaves
Most people don't think about the pharmacy until they need it, but when they need it, they really need it.
Pharmacy users are often sick, anxious, or managing a loved one who is one of those things. They need to get in and get out so they can get back to their lives.
This project was about making identity, consent, and pickup authorization work the way families actually do.
I led registration, dependent and adult linking, pickup authorization, post-registration setup, orders visibility, fulfillment states, and pickup-channel changes. Partners included product, engineering, internal design teams, and legal.
Risk
Failure modes we designed against
The product had to reduce concrete failures: pickup denial, confused caregivers, silent duplicates, and fulfillment surprises when channels are not interchangeable.
- Pickup attempts fail when “family” language hides the gap between managing someone and being allowed to retrieve medication.
- Duplicate profiles scatter prescriptions and weaken authorization decisions downstream.
- Heavy optional tasks during signup steal attention from verification and linking—the highest-risk moments.
- Fulfillment and channel changes break assumptions unless eligibility shows up before patients commit time.
Focus
What I optimized for
- 1. Confirm identity and bind records before exposing household-level pharmacy actions.
- 2. Keep verbs legally precise: separate everyday words (“help,” “family”) from enforced behaviors (manage accounts, respond to invites, pick up).
- 3. Add deliberate pacing where mistakes carry lasting consequences—linking, duplicate handling, consent responses—with recoverable paths.
- 4. Expose preparing, ready, shipped, and inventory exceptions early enough that patients can replan.
- 5. Ship interaction specs—states, empty states, branches—so legal, accessibility, and engineering review the same behavior, not isolated screens.
Decision 1
Verify first, then stage optional work
Constraint: activation pressure competes with safe sequencing. Design pushes verification and membership linkage ahead of insurance, transfers, payments, or managing others.
What changed: sign-in through email verification and profile linkage stay tight; confirmation and a deferrable setup hub follow so patients opt into secondary tasks when ready.
Why it matters: splitting attention during identity steps raises error rates where PHI and guardianship enter the picture.
Decision 2
Explicit permissions and duplicate-record handling
Constraint: disclosure wording and permission boundaries come from legal and privacy—not retail shorthand.
What changed: screens separate account access, management invitations, and pickup allowance instead of folding them under “family.” When the system likely already holds a dependent profile, the flow surfaces conflict, confirms guardianship, and links without silent merges.
Why it matters: fuzzy caregiver language drives counter denial; silent merges fracture prescription history and blur authorization.
Decision 3
Household-aware lists without blurred boundaries
Constraint: mobile density limits clinical detail; the UI still has to signal whose medication each row represents.
What changed: home and orders emphasize prescription ownership, search, filters by household member, and separation between active and completed work.
Why it matters: wrong-household assumptions trigger pickup failure and privacy complaints.
Decision 4
Fulfillment truth and channel limits patients can plan around
Constraint: inventory location, stock, and channel partners set eligibility the interface cannot invent.
What changed: detail views show preparing, ready, and shipped paths; inventory exceptions sit beside in-progress work. Pickup changes expose locker, pay-ahead, and expedited options where eligible. Refill confirmation summarizes split fulfillment when multiple people share one account.
Why it matters: channel switching is where optimism collapses; surfacing limits early prevents wasted trips.
Results
Impact
- ↑ Distinct paths for invites, caregiver responses, and pickup-sensitive actions instead of one vague family affordance
- ↑ Duplicate-record and linking flows route through explicit choices, reducing silent merges across identities
- ↑ Order surfaces foreground inventory-style exceptions next to normal progress so patients adjust plans earlier
- ↑ Pickup-change flows spell channel eligibility, cutting surprises when lockers, pay-ahead, or expedited delivery are not interchangeable
- ↑ Accessibility annotations and analytics events documented per branch—fewer review loops between legal, accessibility, and engineering
Roadmap shifts deferred some launches, but the shipped patterns tighten authorization grammar, make fulfillment states legible, and give downstream teams a shared interaction reference for household-scale pharmacy work.
Next
What I'd push further
Tighter feedback loops between live pickup exceptions and pattern tweaks—especially rushed pickups on shared phones. Next pass: parity polish on invite-expired and pickup-denied branches so stress paths match the clarity of happy flows.
